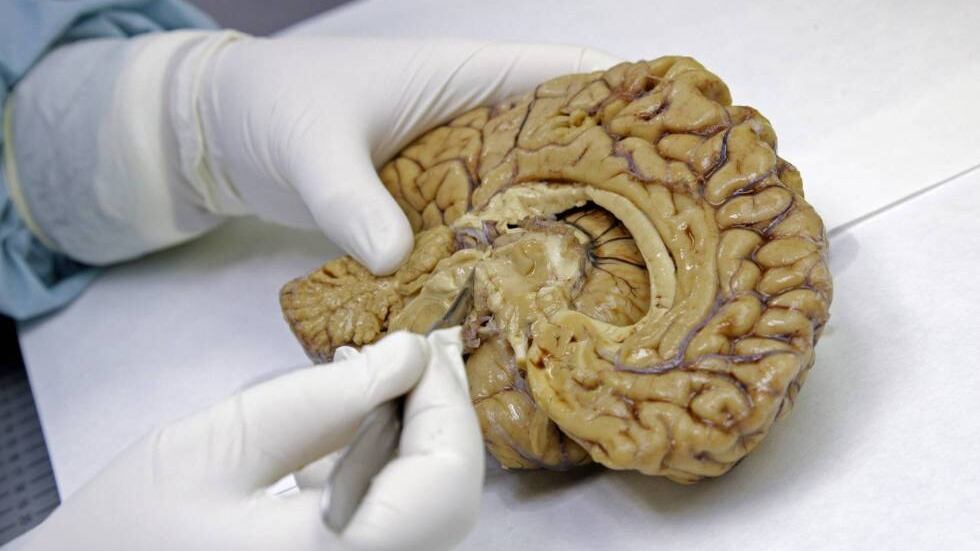
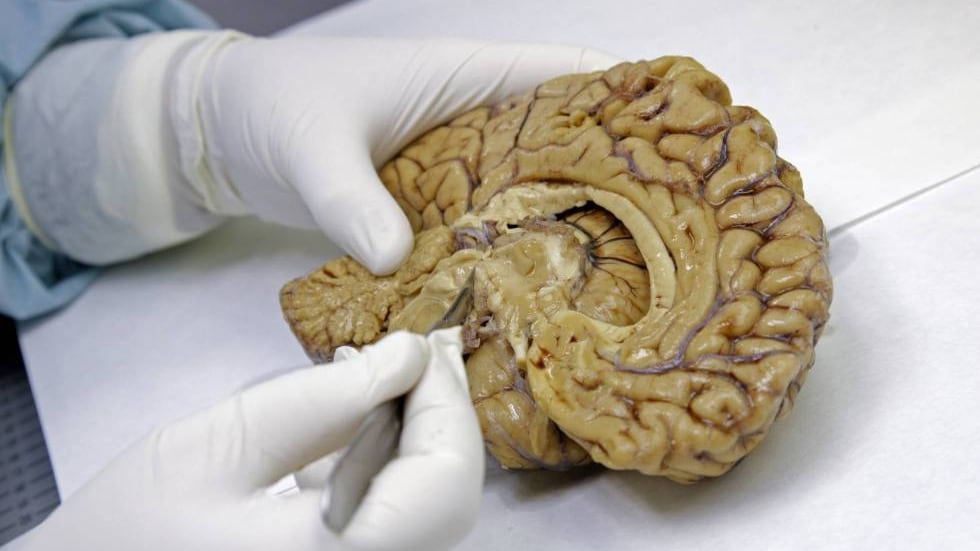
Alzhéimer
Blood Test Can Detect Early Symptoms, 10 Years Before Onset Of Alzheimer’s




Alzhéimer
Longevity Researcher Juan Carlos Izpisua Presents Latest Data On Aging Process: ‘It Is A Loss Of Identity At The Cellular Level’
“If no one asks me, I know what time is. When they ask me, I no longer know,” wrote the philosopher Augustine of Hippo 17 centuries ago. Something very similar happens now with aging: we all understand what it is, but when we ask ourselves why we must age and die, doubts arise. Even the world’s leading experts face the same uncertainty: at best they offer very different answers.
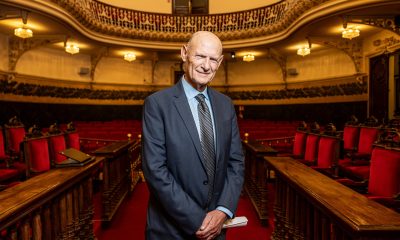
The Spanish biochemist Juan Carlos Izpisua, who has spent decades working in the United States seeking his own answer, has outlined a new view: “Aging,” he says, “is a loss of identity at the cellular level,” and it is possible to recover that identity with experimental treatments. That means aging can be reversed and many of its associated diseases halted.
In 2022, this pharmacologist and biochemist, born in the Spanish town of Hellín 66 years ago, co-founded Altos Labs, where he became its chief scientific officer. It was a new and secretive company funded by some of the richest people on the planet with a $3 billion budget, an unprecedented sum for a biotech start-up.
Alongside Izpisua, other leading figures in aging research such as Pura Muñoz left public institutions to sign contracts with Altos, where salaries can reach €1 million a year. Four Nobel laureates followed the same path. The company’s goal was unusual: it was not looking for a pill against aging, but rather to do basic science aimed at rejuvenating human cells and, in doing so, curing age-related diseases such as cancer and Alzheimer’s, among many others.
On Wednesday, Izpisua took the lectern in the auditorium of Spain’s Royal National Academy of Medicine, just a few steps from the Royal Palace in Madrid, to give a lecture unpacking his latest scientific results, including some that will be published in the coming days. The session was organized by the Catholic University of Murcia, with which Izpisua has collaborated for a decade.
The main idea is that human cells work brilliantly from before birth, when we are an embryo of barely a week, until we reach roughly 30 years of age. “Until then, if you don’t have a genetic disease or suffer an accident, you don’t need to see a doctor,” the scientist said in the academy’s auditorium, crowned by portraits of some of history’s greatest physicians and just a few steps from the chair once occupied by Spanish Nobel laureate Santiago Ramón y Cajal. It is after what he calls “the first wave of aging” that, according to Izpisua, cells begin to lose their identity. It is as if their functions blur and they stop behaving as they should. Over time, the stress response of these cells ceases to be optimal, and they transform into senescent old cells that give rise to fibrosis, which is the cause of many age-associated diseases.

For Izpisua, this phenomenon answers why we age. Its scientific name is epithelial–mesenchymal transition, a fundamental process that allows cells to migrate during embryonic development and generate the different organs that will form the body — the famous gastrulation, the most important moment in a person’s life. But in adulthood, this process is the most deregulated in more than 50 human diseases, the Altos researcher said in his lecture. This loss of identity “is the first measurable sign of aging,” he emphasized, ahead of mitochondrial deterioration — the cell’s energy engine — or telomeres, which protect DNA from damage.
This loss of identity spreads through the body via the bloodstream and takes hold in other organs, according to his latest research. In a study using the UK Biobank, which holds biological samples from more than half a million volunteers, his team found that blood proteins linked to this loss of identity are those most strongly associated with mortality. “We have analyzed a large number of human diseases as well as all organs during aging, and what we observe is this cellular drift defined by a genetic transcriptional signature that leads to a loss of cellular identity,” he explained.
The researcher has developed an experimental intervention to reverse this phenomenon. It is called partial cellular reprogramming and is inspired by the work that gave the Nobel Prize in Medicine to Shinya Yamanaka, who also works for Altos. Yamanaka showed that activating four genes is enough to transform an adult skin cell, for example, into an embryonic stem cell capable of forming any tissue in the body. For the first time, it was possible to roll back the developmental and aging clock.
In experiments with mice, Izpisua has observed that partial cellular reprogramming — an intervention similar to Yamanaka’s but limited in time to two days per week of reprogramming — extends lifespan. It also reverses, for example, liver and metabolic damage associated with high-fat and high-calorie diets in animals with congenital obesity. The intervention also regenerates damaged muscle; other labs have reported similar rejuvenating effects in the brain, heart, eyes, kidneys, pancreas and liver. “A single intervention has effects across the organism,” Izpisua reasoned. “We are touching the heart of the process that gives rise to disease,” he summarized.
The scientist is realistic: introducing this treatment in humans is possible but much more complicated. First it must be ensured that partial reprogramming does not cause harm, above all the most feared outcome: the emergence of tumors if the rejuvenation process goes beyond what is intended. “We have treated more than 7,000 mice and in no case have we seen differentiation into an embryonic cell,” the scientist said.
Before moving to experimental treatments for patients, Izpisua has begun applying partial reprogramming ex vivo. He will do so with donated organs deemed unsuitable for transplantation. The experiment, carried out in collaboration with Hospital Clínic de Barcelona, will apply partial reprogramming to damaged viscera to see if it can repair some of the accumulated damage. “We know a mouse is not a human, but we have to start somehow applying this to people,” the researcher said.
Sign up for our weekly newsletter to get more English-language news coverage from EL PAÍS USA Edition

The Rising Cost Of Finding Love

Luxury Villas For Sale, Estepona – ProjectL1

Tourist Begs Police Not To Fine Her After Swimming In The Trevi Fountain During Heatwave




-
blackout April 20253 weeks ago
Insurance company Mapfre decides to pay out €14 million compensation for 2025 blackout
-
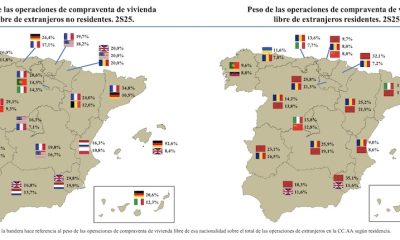
 Foreign demand3 weeks ago
Foreign demand3 weeks agoWho Bought Where In The Second Half Of 2025?
-
 New Developments4 weeks ago
New Developments4 weeks agoStylish 3-Bedroom Apartment With Panoramic Sea Views – Benalmádena
-

 New Developments3 weeks ago
New Developments3 weeks agoInside The Most LUXURIOUS Apartment Building In Spain!
-
Costa Blanca South3 weeks ago
Alicante police chief to retire after 17 years of service
-

 New Developments3 weeks ago
New Developments3 weeks ago🌅 Stunning Penthouse With Panoramic Sea & Mountain Views Benalmádena
-
biggest ever cocaine bust4 weeks ago
Spain’s biggest-ever cocaine bust – massive Atlantic seizure stuns authorities
-

 Uncategorized4 weeks ago
Uncategorized4 weeks agoAudi F1 star