Africa
The Trump‑blocked Contraceptives That Never Reached Kenya: “I Am Not Ready To Have Another Baby”

In a huge warehouse in Geel, Belgium, $9.7 million in contraceptives have been locked up since early 2025. Some 77% of the shipment from the United States Agency for International Development (USAID) was destined for about 10 African countries, including Kenya, Nigeria, the Democratic Republic of Congo and Mali. But when Donald Trump’s administration dismantled the world’s largest development aid organization, these medicines were left stranded, destined either to be destroyed or to expire box by box. About 5,800 miles south of Belgium, in Nairobi, the capital of Kenya, Jane Anyongo, Violet Mosomi, Salma Kamau, and hundreds of thousands of women are still waiting for their pills, condoms, subdermal implants, intrauterine devices, and other sexual and reproductive health supplies.
“I have to be patient,” Anyongo tells herself beside the maternity ward of the public health center in Embakasi, near the capital’s airport. It is May 2026. For three years, she has had a subdermal implant in her arm — a small contraceptive rod that releases hormones to prevent ovulation. It expired a month ago, but she has been unable to replace it because there are no supplies. She is 27, has two children, and does not want any more. Like her, 76% of married women in Kenya aged 15 to 49 want family planning. In this East African country, modern contraceptive use is 57%.
“But I couldn’t find the three‑year implant or the five‑year one,” Anyongo says. And her next appointment with family planning staff is still some time away. “If by then I still haven’t got one, I’ll switch methods.” But choosing an alternative is not easy.
Anyongo cannot afford to buy an implant with the income from her small business. The device alone would cost about 1,500 Kenyan shillings (around $12), plus the cost of the health care visit. She says that if she has no choice, she will resort to oral contraceptives. What she does not know is that those are also in short supply in Embakasi and that the health center has not been able to provide combined oral contraceptives to any patient since January.

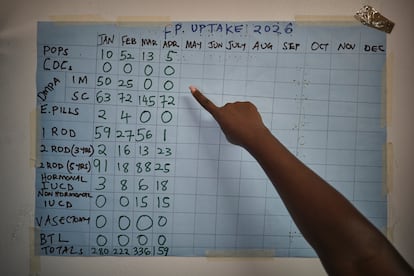
Brenda Onyango, deputy head of the maternity department at the Embakasi health center, walks into the medicine storeroom and points to a chart drawn by hand with markers. The different contraceptive methods are lined up, and each month of the year occupies a column. This is how they record how many women access each method.
“Zero means there is no stock,” she explains. The row for Combined Oral Contraceptives (COCs) shows zero for every month of 2026, and the space for the morning-after pill is also empty in March and April. For the others, such as intrauterine devices (IUDs) or subdermal implants, a worrying irregularity can be seen in recent months.
“We suggest they use other methods because we want to avoid unwanted pregnancies. But most are reluctant,” Onyango adds in an interview with EL PAÍS, referring, for example, to injections that provide protection for up to three months or other long-acting methods. However, when it comes time to decide, misinformation or bad experiences they have heard from other women weigh heavily.
Rise in pregnancies
The effects of these shortages are already becoming visible, and unplanned pregnancies are increasing. “Our post‑abortion care services have increased by 50%. Last year we barely saw about 10 cases a month; now we reach 15 or even 20,” she laments.
Most patients are aged 19 to 24 and have undergone abortions outside the health system. In Kenya, the Constitution permits voluntary termination of pregnancy in two cases: when there is a medical emergency or the mother’s life is at risk.





At the Embakasi outpatient clinic, they also prescribe contraceptives to women who have just given birth. On average, they handle about 70 deliveries a month. “But in April we could only provide for 20,” Onyango says.
More than 1.4 million women worldwide will be affected by a decision made in the United States that blocks distribution of contraceptives already purchased. In Kenya, 108,000 women will be left without access to implants — 13.5% of annual demand — according to MSI Reproductive Choices’ office in the country.
This NGO, together with Kenya’s public health system, is also affected by disruptions to USAID contraceptive supplies, which remain stored in a warehouse in Belgium. One hundred percent of the supplies MSI distributed to public health centers — such as Embakasi — came from USAID and the United Nations Population Fund (UNFPA). “They also supplied 65% of the contraceptives offered in the private system,” says George Mbugua, the head of public sector strengthening and outreach at MSI Kenya.
But MSI Kenya not only did not receive the implants and other contraceptives stranded in Belgium; it also did not immediately receive some consignments that did arrive in Nairobi. “Part of the stock was initially held at the Kenya Medical Supplies Authority [KEMSA], the government’s warehouse, due to USAID budget cuts for its distribution,” Mbugua adds.
Because of shortages and supply problems, the NGO has had to buy on the local market, Dr Walter Obita, director of MSI Kenya, explains. That has made the service slightly more expensive for public‑sector patients and for those attending private clinics. “Previously, the product was free, and we only charged for the service. Now, in some cases, we have to charge for both,” Obita says from MSI’s Nairobi headquarters.
For example, Sayana, an injectable contraceptive that protects for up to three months, used to be supplied free by the Ministry of Health. MSI Kenya only charged 100 shillings ($0.70) to each patient for the first application and counselling. But when it has to buy it on the local market, the cost rises to 300 shillings (about $2.33). In vulnerable areas, the NGO charges women only for the product and provides professional counselling for free; in wealthier areas it bills those 300 shillings plus 30% for counselling.
The U.S. was the largest donor of family planning services and supplies. According to a study published in The Lancet Global Health, the closure of USAID will leave 100 million people in 41 countries without access to contraceptives over the next five years. This could lead to up to 55 million unplanned pregnancies and about 20 million abortions, 75% of them in unsafe conditions.
Separately, the U.S. and Kenya signed a new bilateral global health agreement in December, the new form of foreign aid promoted by the Trump administration. However, the 37‑page document does not mention family planning, nor does it explicitly list contraceptives among its supplies or targets. It does, however, incorporate the Helms Amendment, a 1973 law which prohibits the use of U.S. funds “to pay for the performance of abortion as a method of family planning or to motivate or coerce any person to practice abortions.”
In the last year, Washington has signed 22 such bilateral agreements with African countries. Yet experts have questioned the new health priorities, the handling of health data and the conservative policies on sexual and reproductive health services.
Destroyed or allowed to expire?
The scandal over the contraceptives stored in Belgium erupted last year when it became known that the U.S. had ordered the shipment to be incinerated in France. Washington said it was merely applying the so‑called “Mexico City policy,” approved in 1984 and known as the global gag rule, which bars foreign organizations that provide, counsel on or promote legal abortion services from receiving U.S. foreign assistance. Belgium’s Foreign Ministry confirms that part of the shipment remains in Geel and that another portion has been stored in the town of Kallo. “We continue to work to find a solution,” a spokeswoman said by email.
MSI Reproductive Choices has offered to store and redistribute the contraceptives at no cost to the U.S. According to its calculations, about 362,000 unplanned pregnancies, 110,000 unsafe abortions and 718 maternal deaths could be prevented in the various countries of the Global South to which they were destined.
Doctors of the World and Médecins Sans Frontières (MSF) have also offered to redistribute the supplies. But The New York Times, citing an internal USAID memorandum, reported that only 17% of the contraceptives remained usable in September 2025.
Belgium’s Foreign Ministry and MSF told EL PAÍS that they had not seen that USAID document directly. “We need more clarity on the condition of the supplies before we can accept and facilitate their transfer. It is deeply troubling that these essential and potentially life‑saving contraceptives remain in storage months later,” Mihir Mankad, director of Advocacy and Global Health Policy at MSF USA, told this newspaper.
In early April, various organizations staged a protest outside the Geel warehouses to demand that the Belgian government and the European Union prevent the destruction of the supplies and support their redistribution.
EL PAÍS contacted the U.S. State Department and the communications office that still handles queries about the programmes that were run by USAID, but did not receive a response.
While the fate of family planning supplies is being decided in the Global North, in Embakasi, Violet Mosomi is waiting for her pills. She is 25, became a mother at 17, and wants to avoid another pregnancy. “If I had known at school about family planning and that I could decide whether I wanted to be a mother, I would have chosen not to be one,” she says.
Mosomi started taking the pill and in 2023 switched to an IUD, but she experiences side effects. “It gives me fever and nausea, I feel weak and sometimes I don’t even get my period,” she says. “My nurse has suggested I change method. I want to use pills; they suit me better,” she adds.

Juliana Kingoro, a community health worker in Embakasi, knows Violet’s case and those of many other neighbourhood women and confirms that it just isn’t financially viable. “For example, a Jadelle [subdermal implant] costs 2,700 shillings [almost $21] in a private hospital. If you are forced to buy it, how do you pay the rent or buy food for the children?” asks Kingoro, who has worked since 1992 in Nairobi’s neighborhoods advising women on contraceptive choices.
“People do not have access to family planning, but they need it. Given the economic situation, our people do not want children or at least try to space them. If we control population growth, everything would improve: women could access work, children would attend school and the population would be healthier,” she tells EL PAÍS.
Kingoro is responsible for 120 households that she visits each month. On her cell phone, she records follow‑ups for each woman using a Ministry of Health application. “But since USAID cut aid, we have no condoms to give to young men nor pills for adolescents,” she says. In Kenya, the teenage pregnancy rate had fallen from 18% in 2014 to 15% in 2022.

Although Kingoro refers patients to health centers to access long‑acting contraceptive methods, she cannot guarantee they will find them. Some women have lost interest in family planning and no longer open their doors when she visits. “Others turn to herbal remedies or, in emergencies, to the P2 [Postinor‑2 or morning‑after pill]. In the long term, this can affect their health or prevent them from having children,” she says.
‘We are not going anywhere’
Queenter Onyango, a liaison between organizations and Kenya’s Ministry of Health, acknowledges that the suspension of USAID has deeply affected the outreach work carried out by community workers like Kingoro.
“We manage with what we have. But we remain open to working with other partners because we cannot be stuck because of the cuts,” says Onyango.
For his part, the director of MSI Kenya agrees that USAID’s closure has had a negative impact on the public‑sector staff they worked with. “Some were paid from USAID funds. With the cuts, those jobs were lost: people we had trained to strengthen the system. Where there used to be three or four people providing long‑acting family planning services, now only one remains,” he says.
MSI Kenya is currently working to present alternative financing options to Parliament while trying to maintain access to contraceptives and care at affordable prices. “These changes force us to adapt so every woman can continue to choose. But we are not going anywhere,” stresses its director, Walter Obita.
Margaret Mwawa, director of the Njiru health center in Nairobi, and Dorothy Ndeje, head of the family planning unit, search through a drawer for the last remaining contraceptives donated by USAID. On the clinic’s window frame hangs a rudimentary chart tracking supplies distributed during 2025. The pills show “zero” throughout the year, and other methods began running out from May onward. “We haven’t had copper IUDs for two months,” they say.
And Salma (a fictitious name) is looking for precisely that contraceptive method. She is 32, has four children and wants to stop taking pills. Although she can get them for free in Njiru, they are rarely available and on several occasions she has had to ask her husband for money to buy them. “I am not ready to have another baby,” she says.








Africa
Hungry Elephants Displaced By The Climate Crisis With Farmers For Food In Zambia: ‘They Ate The Maize The Whole Night’

Veronica Akabondo had worked from dawn to dusk for months on her farm in southern Zambia and was confident she would have a plentiful maize harvest. But one morning she woke up and found it all gone. The culprit? A herd of hungry elephants.
“They came and ate the maize the whole night,” Akabondo says, distraught, standing in the trampled remains of her field. “They finished everything. Even the pumpkins I had planted in the same field were not spared,” adds the 60-year-old woman.
Akabondo lost about 6,000 kilograms of maize in one night, the equivalent of $2,700. She now wonders how she will support the eight children in her care. The woman’s farm is in Livingstone, a town that straddles Mosi-oa-Tunya National Park. The area, which opened in 2012, is part of the Kavango-Zambezi Transfrontier Conservation Area, between the rivers of the same names, and is the world’s largest transboundary conservation zone, covering an area larger than Spain. This vast mosaic of 36 protected areas, national parks and wildlife corridors spans Angola, Botswana, Namibia, Zambia and Zimbabwe, and aims to provide safe migratory routes for the region’s more than 200,000 elephants, the largest population of these mammals in the world.
In recent years, Zambia — one of the poorest countries in the world, where more than 60% of its 21 million people live below the poverty line — has been hit by extreme weather events that have reduced harvests and worsened malnutrition. Today, roughly one-third of Zambian children under five have stunted development due to poor nutrition. Severe droughts combined with extreme flooding have also led to a rise in violent clashes between people and elephants. Displaced from their usual migratory routes, these animals trample crops in search of water and food, at times causing deaths and plunging families into destitution by leaving them without their livelihood. As a result, some farmers have killed elephants that enter their fields.
A devastating cost
According to the United Nations Development Programme (UNDP), such incidents were once rare, but since the drought began in Zambia “more and more elephants are venturing out of Mosi-oa-Tunya National Park in search of water and food.” “For the animals, particularly the elephants, this is a matter of survival. Their water sources have dried up, and their typical food sources are dwindling. The effects of the drought are further compounded by increased elephant populations, as elephants from Botswana, Zimbabwe, and Namibia have migrated into the national park,” states a 2025 UNDP report, which says this “desperate” search for resources takes a devastating toll on humans.
More than 50 years ago, elephants moved freely on both sides of this border, which existed only on maps and was covered in dense vegetation. Today, it has been replaced by farmland within the Transfrontier Conservation Area (TFCA) established by Zambia and Malawi in 2015.
In 2022, the Malawian government reintroduced 263 elephants to Kasungu National Park, on the border with Zambia. Since then, there have been several clashes between animals and humans in the area, with at least 10 deaths linked to these encounters, not including the destruction of dozens of hectares of crops.
Elephants are also appearing much earlier than usual, and especially before farmers have harvested their crops. “In the past, elephants appeared around May to July. But this time they came while crops were still in the fields,” says 53-year-old Kennedy Muleya.
Like Akabondo, Muleya’s maize was destroyed in February by a herd of hungry elephants. It had never happened to him before. “It was during the night, so we could not go to the field because it is dangerous. Elephants can kill,” Muleya recalls. “When we went in the morning, we found everything destroyed. This is the food we depend on. Now we have nothing.”

The search for food
Rwinick Mapanza, president of the Livingstone District Farmers’ Cooperative Union, believes the heavy rains — which produced abundant fresh vegetation — likely drew elephants into Zambia in search of food, as it is a territory they prefer during wetter seasons due to its higher elevation. “These animals know where food is found,” says Mapanza.
But even knowing what drives them to these areas, it is very difficult to control them. Farmers have tried banging cans to make noise, lighting fires and using clothing soaked in chili mixed with grease — a cheap and harmless method that repels the mammals, which are highly sensitive to pepper that irritates their trunks. But it is often too late.
“Once elephants get into the fields, the damage is done,” says Wilfred Moonga, a ranger with Zambia’s Department of National Parks and Wildlife (DNPW).
Farmers are frustrated because so far they have received no compensation for lost crops nor any subsidies to help them protect themselves more effectively from elephants.
Akabondo says some government officials visited her ruined field and took photographs, but nothing has been done since then. “We are asking the government to help us because we are really suffering,” the farmers say.
When farmers reported the crop destruction to the DNPW, they were simply told to hire guards. Aside from the cost this entails, Akabondo rejects the idea, arguing the elephants are too dangerous. “We would be putting lives at risk,” she says.
Sign up for our weekly newsletter to get more English-language news coverage from EL PAÍS USA Edition


Seis Personas Apuñaladas En La Principal Estación De Tren De Nueva York Horas Antes De La Visita De Trump
The Experts’ Tips For Staying Safe While Hiking In Spain’s Mountains
Los Agricultores Andaluces Piden Que Vox No Asuma La Cartera De Agricultura En Las Negociaciones Para La Investidura De Moreno

How To Get A Tourist Rental Licence In Andalusia (Spain) – Step-By-Step Guide 2025
Spain heatwave 2026: When the next extreme temperatures could hit and which areas may suffer most

FBI investigation launched over Valtteri Bottas Cadillac theft






-
 New Developments3 weeks ago
New Developments3 weeks agoHow To Get A Tourist Rental Licence In Andalusia (Spain) – Step-By-Step Guide 2025
-
aemet3 weeks ago
Spain heatwave 2026: When the next extreme temperatures could hit and which areas may suffer most
-
 Uncategorized4 weeks ago
Uncategorized4 weeks agoFBI investigation launched over Valtteri Bottas Cadillac theft
-

 Uncategorized3 weeks ago
Uncategorized3 weeks agoMax Verstappen is no diva – Nurburgring rival on
-
Costa Blanca South4 weeks ago
Torrevieja opens registration for Concilia Verano 2026 summer school
-
Costa Calida4 weeks ago
Puerto de Mazarron prepares for San Isidro festivities with music and traditions
-

 Argentina2 weeks ago
Argentina2 weeks agoTrump Receives Flávio Bolsonaro In The Oval Office Three Weeks After Lula
-
A-7 motorway3 weeks ago
Wrong-way kamikaze driver dies in horrific head-on collision on Marbella A-7 motorway